

No products
To be determined
Shipping
0,00€
Total
Product successfully added to your shopping cart
Quantity
Total
There are 0 items in your cart.
There is 1 item in your cart.
Total products
Total shipping
To be determined
Total
Methods of treatment in case of Nervous Mandibular is Injury caused by Dental Implant
Punching of the inferior dental canal has the second place concerning the rate of its arising after punching of the genyantrum bottom with applying of dental implantation. The understanding of process of conditioning the development of complications linked with mechanical compression of nervus mandibularis allows to work out the inference about necessity of early use of any methods of treatment. It means that precautions of possible complications are getting some prevalence which turns into cause of growing alarm of implantologists.
So object of our research is the detection of the best medical approach and performance after appearance any signs and symptoms of paresthesia in case of implantation side part of lower jaw.
aterials and methods
Twenty patients had complaints concerning reduced skin sensitivity on their chins, lower lips and anterior teeth in postsurgical period after surgical placing of implants was chosen as a subject of the research. The age range among patients is from 23 to 68 years. The zones of temperature, tactual and pain sensitivity were observed among all patients during the whole course of study. The computer-aided tomography has revealed implant contiguity to inferior dental canal of punching of upper wall of the canal (photo 1 and 2).
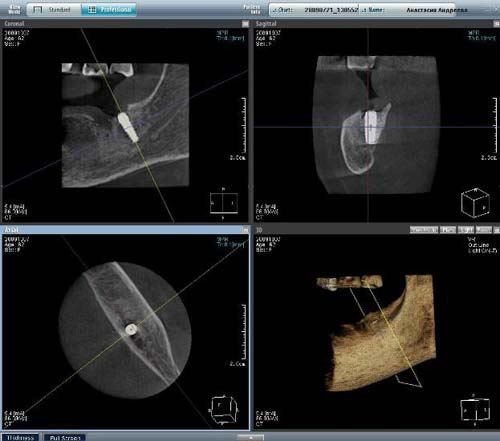
Photo 1. Canal wall perforation.
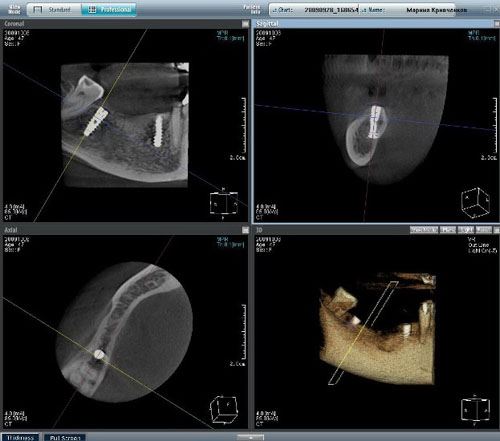
Photo 2. Nerve compression with the implant
The outcome and its discussion
The atrophia of alveolar process altitude, the inferior dental canal is located on the distance from 5 to 7 mm from alveolar crest. The process of placing of screw-like implants in such zone is fraught with punching or compression of nervus mandibularis The canal is crossed by this nerve and an artery. The punching of canal wall is conjugated with arterial bleeding which is easy to stop with tight swabbing or input of absorbable gelatin sponge into the bone wound. The implant put in this place makes a case of neural compression for account of forming of intracanal hematoma. Composite traditional treatment was applied but appeared to inefficient for all the the patients regardless of duration and drugs. The relief was reached only by disposal of implant. The pain disappeared right when the implant was put out. The expected management appeared to be fallacious. When the tip of the implant was situated in 1-2 mm from top wall of canal the tactual sensitivity kept against the background of revealed ache and temperature ones. The renewal of sensitivity after disposal of the implant took from five to eight weeks but only in cases when the implant was disposed not later than within ten days since arrival of paresthesia. Mandibular nerve has high regeneration capacity but it's impossible to avoid neural excision in case of violation of rules of preparing of osseous tissue with atrophy of the lower jaw results in constant paresthesia. The fallacious expected management used by us involved profound neural regenerative changes which declared themselves in constant vanishing of sensitivity.

Photo 3. Localization of canal when height atrophy.

Photo 4. Damage of canal with cutting instrument leads to formation of intracanal hematoma.

Photo 5. Intracanal hematoma.
The inference
Long-range inefficient traditional treatment of patients with obvious worsening of neural function allows working out the conclusion that there's no opportunity to get rid of paresthesia without disposal of implant. In disputable situations there's a need in specializing the implant localization with the assistance of computer-aided tomography. After the localization is confirmed in the canal lumen the fastest disposal of the implant is necessary.